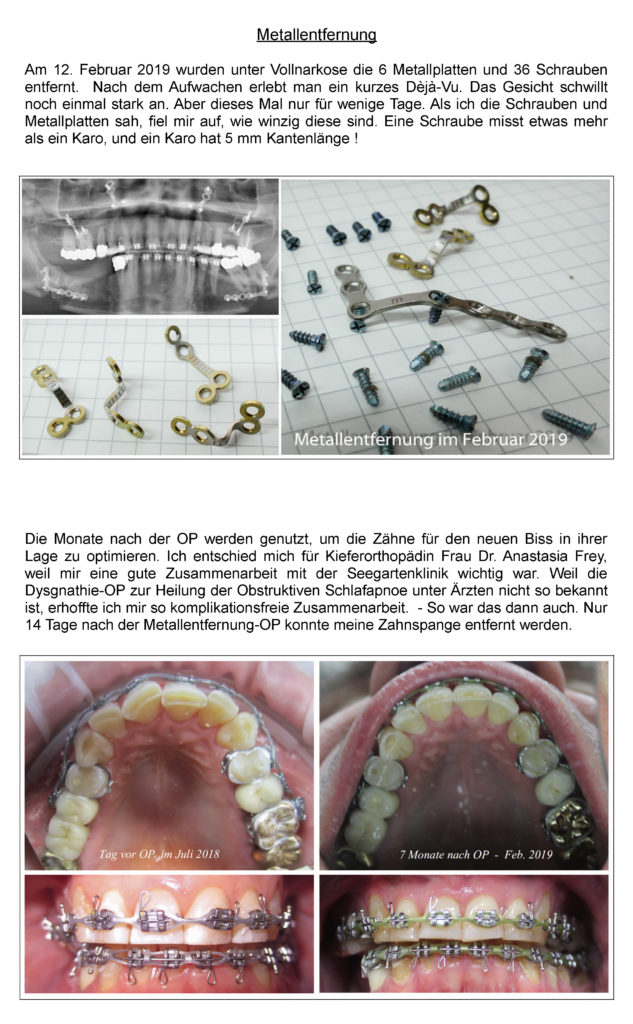
-
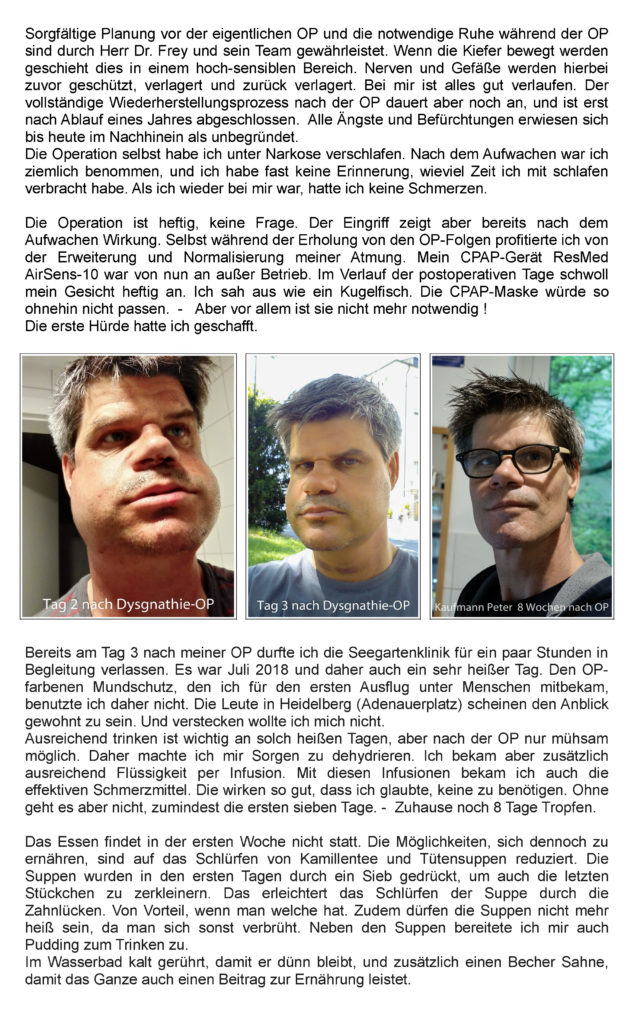
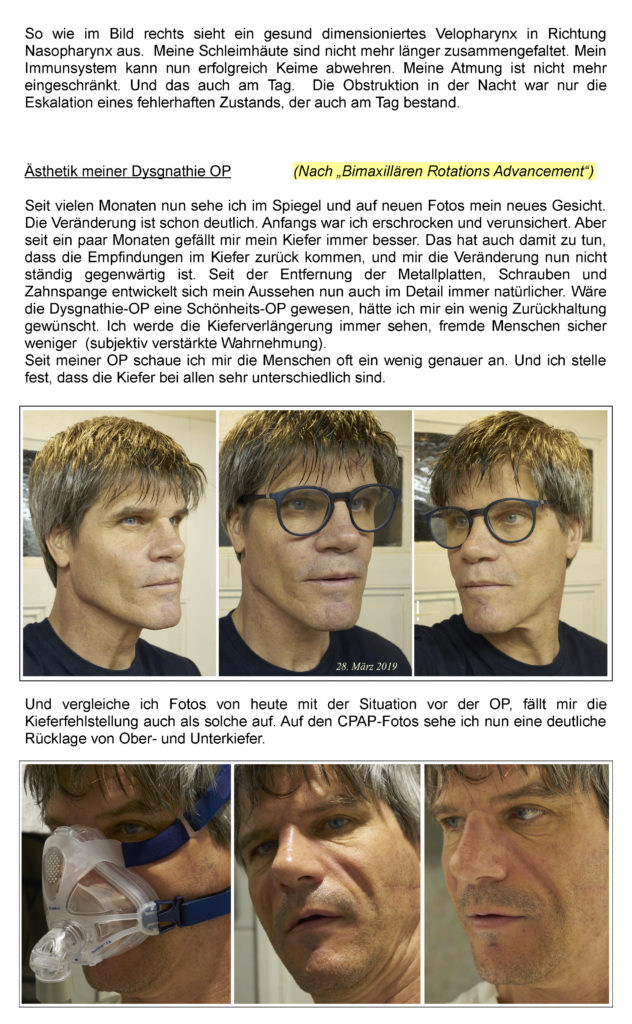
Vor der Schlafapnoe Operation
Vor der Schlafapnoe Operation
Heute ist der 1. März 2019, und es geht mir gut. Meine OP war am 11. Juli 2017. Ich bin froh darüber, mich für die Schlafapnoe Operation in der Seegartenklinik entschieden zu haben. Bereits seit vielen Monaten kann ich wieder durchschlafen. Das Einschlafen vollzieht sich zügig und ohne Herzrasen. In den Jahren vor der OP erhöhte sich mein Puls nach dem zu Bett gehen bis hin zu Herz- Rhythmus- Störungen, weil meine Atmung aufgrund verengter Atemwege erheblich behindert war. Jeder Atemzug war um 50 % im Fluss limitiert. Immer kurz vor dem Einschlafen schreckte ich auf. Der Herzschlag war erhöht und ging nur zögerlich auf Normalpuls zurück. Das Einschlafen war so fast unmöglich. Aber weil jeder irgendwann schlafen muss, schlief auch ich dann nach Stunden ein, um im Schlaf dann 153 mal durch körpereigene Weckreaktionen des Gehirns (CO2Anstieg) aus dem Schlafrhythmus gebracht zu werden. Erholsamer Schlaf ist so unmöglich. Am Morgen wurde ich nur sehr zögerlich wach bzw. dämmerte so vor mich hin, ohne richtig das Bewusstsein zu erlangen. Erste Polygraphie (PG) im Mai 2017.
-
Von der Schlafapnoe geheilt
Von der Schlafapnoe geheilt
Heute ist mein Schlaf erholsam, und ich träume wieder sehr viel und zusammenhängend. Die Hypopnoen und Apnoen sind auf Null zurückgegangen. Auch das Schnarchen ist völlig verschwunden. Vor der OP und auch unter CPAP-Therapie war das nicht der Fall. Meine Leistungsfähigkeit am Tag ist erheblich gestiegen. In der 9. post-operativen Woche begann ich wieder mit dem Radfahren und dem Schwimmen. Während des Schwimmens zeigt sich die Verbesserung vom ersten Meter an. Ich schwimme sofort die 3-fache Distanz gegenüber vor der OP. Beim Schwimmen liegt der Körper tief im Wasser, die Atmung muss nun beim Einatmen auch gegen den Wasserdruck arbeiten. Durch die Erweiterung meiner Atemwege um 250 % im Querschnitt (an der engsten Stelle) gibt es nun beim Ein- und Ausatmen keinen Widerstand mehr. Die Luft strömt einfach so rein und raus. Das Gefühl unter zu gehen ist weg.
Aber auch im Alltag verspüre ich die Verbesserung vom ersten postoperativen Tag an. Bereits 14 Tage nach der OP konnte ich den Weg vom Hauptbahnhof Heidelberg zur Seegartenklinik mit geschlossenem Mund laufen, ohne Atemnot zu spüren. Meine Atmung ist wieder normal. Bis vor der OP musste ich bei der geringsten Anstrengung durch den Mund atmen und hob ihn dabei an, weil ich nur so ausreichend Luft bekam.
-
Die Ursachen meiner Schlafapnoe
Die Ursachen meiner Schlafapnoe
Seit meinem Geburtsjahr 1965 bin ich Nichtraucher und trinke keinen Alkohol. Aktuell 53 Jahre alt. Mit einer Körpergröße von 185 cm und 77 kg Gewicht ermittelt sich ein BMI von 22.5 BMI-Rechner im Internet: Super! Ihr Gewicht ist gesund. Mit einer ausgewogenen Ernährung und regelmäßiger Bewegung wird das auch langfristig so bleiben.
Eine erste Polygraphie 2017 zeigte eine schlechte Schlafqualität, viele Weckreaktionen, zentrale und obstruktive Apnoen, Hypopnoen, sowie Phasen einer Cheyne-Stokes-Atmung. In einer Polysomnographie 2018 (Schlaflabor) wurde ein Obstruktives Schlafapnoe Syndrom mit einem AHI von 18.5 ermittelt. Wenn Übergewicht ein großer Faktor für einen hohen AHI ist, wie muss dann ein AHI von 18.5 bei einem BMI von 22.5 beurteilt werden? Nun, ich kann mein Gewicht nicht reduzieren, um meine Situation zu verbessern, es muss daher einen anderen Grund für die Obstruktion geben.
-
Die Schlafapnoe Operation
Die Schlafapnoe Operation
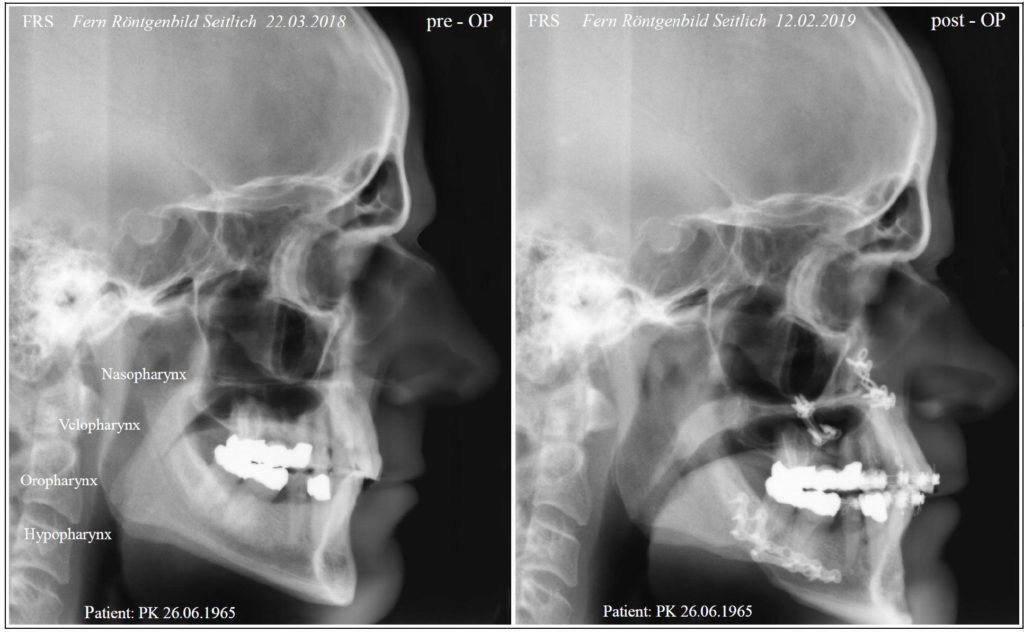
Während einem langen intensiven Gespräch erklärte mir Herr Dr. Frey mit Zuhilfenahme eines FRS (Fern-Röntgenbild-Seitlich) die Situation, meine Situation. Ich verstand jedes Wort und mir war sofort klar, dass nur diese Operation Heilung bringen kann. Und der Begriff Heilung ist hier wirklich angebracht.
Eine Kiefer-OP zur Behandlung der OSA stellt den Zustand wieder her, wie er eigentlich richtig ist, um Gesundheit und Leben zu erhalten. Die OP dreht ein Stück Evolutionsgeschichte einfach wieder zurück. Der Eingriff heilt daher die Obstruktive Schlafapnoe. Und das nicht nur für die Zeit des Schlafs, sondern für den ganzen Tag, für mein ganzes künftiges Leben. Ich bin in der glücklichen Lage noch keinen Herzstillstand mit Infarkt als Folge gehabt zu haben. Jeder Interessierte kann sich in den Videos von Dr. Frey (im VideoBlog oben / oder in YouTube) diese medizinischen Fakten hervorragend erklären lassen.
-
Entscheidung für die Schlafapnoe Operation
Entscheidung für die Schlafapnoe Operation
Nun gab es nur noch eine Hürde, die Entscheidung für eine solche Operation. Die Operation ist schwierig und kostet Geld. Ich habe mir für die Entscheidung einige Wochen Zeit genommen. Parallel zu meinem ersten Gespräch mit Herr Dr. Frey war ich für eine alternative OSA-OP in Karlsruhe angemeldet (UPPP). Im Internet habe ich mich zudem nach weiteren Alternativen umgeschaut – es gibt keine. Einen Tag vor der geplanten UPPP in Karlsruhe wurde die OP vom HNO-Chirurgen verworfen, da eine Beschneidung (plastische Umgestaltung) meines Gaumensegels und der Nasen-scheidewand meinen Atemwegsquerschnitt nicht vergrößert hätte. Das ist aber notwendig.
Auch die CPAP-Anwendung kann meinen Atemwegsquerschnitt nicht verlässlich offen halten, und schon gar nicht vergrößern. Eine Protrusionsschiene wirkt nur auf Höhe des Hypopharynx auf die Weichteile ein. Die Engstelle in Höhe meines Velopharynx wird durch sie nicht therapiert. Langfristig in Anwendung kann die Protrusionsschiene sogar erhebliche Nachteile auf die Verengung haben, da sie eine Kraft auf den Oberkiefer ausübt. Das ist kontraproduktiv.
Sehr geholfen haben mir die Patientenberichte der Seegartenklinik. Ende Mai 2018 entschloss ich mich daher noch einen Schritt in Richtung OP zu gehen. In der Seegartenklinik wurde eine Digitale-Volumen-Tomographie zur Planung meiner OP erstellt.
-
Empfehlung zur Schlafapnoe Operation durch das Klinikum Karlsruhe
Empfehlung zur Schlafapnoe Operation durch das Klinikum Karlsruhe
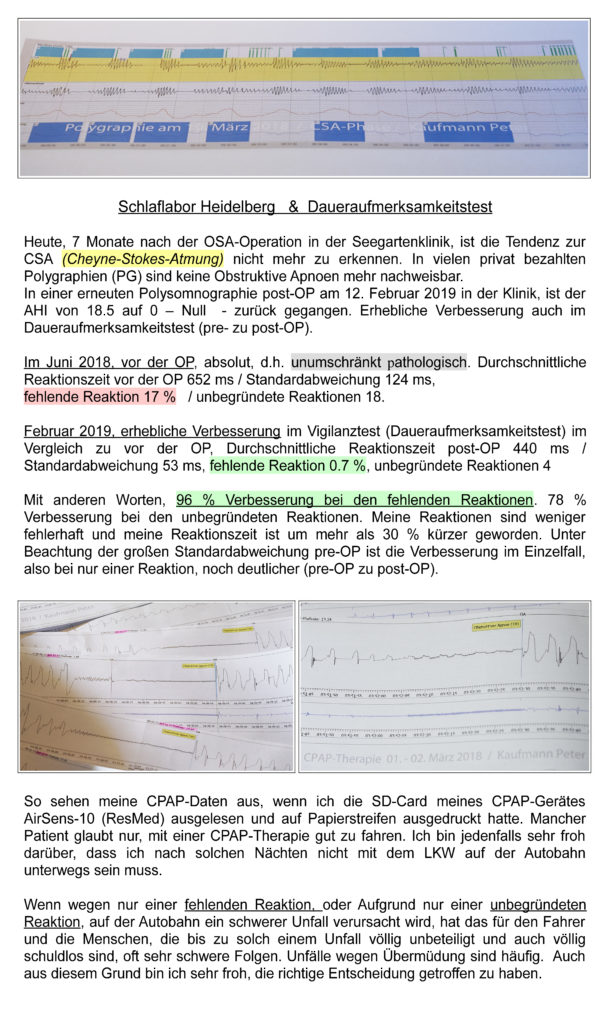
Im Januar 2018 wurde während einer stationär durchgeführten Polysomnographie in Karlsruhe mehrfach eine Blutgasanalyse durchgeführt. In meinem Blut war auch am Tag der pCO2 Wert zu hoch (über dem Grenzwert für Kohlenstoffdioxid), und der pO2 Wert unter dem Grenzwert für Sauerstoff im Blut. Mit anderen Worten, der Gasaustausch war auch tagsüber gestört und erklärte sehr gut die anhaltende Müdigkeit über den ganzen Tag. In der Nacht zeigte sich diese Spreizung der pCO2 zu pO2 (Sauerstoffpartialdruck) in der Tendenz zu einer Cheyne-Stokes-Atmung. Mehrfach wurde die CSA in Polygraphie und unter CPAP-Therapie beobachtet und dokumentiert. Während jeder Polysomnographie klagte ich dem Arzt, ich würde nicht genug Luft bekommen. Selbst nach einer PSG, stationär im Krankenhaus, wurde aber keine einfache flexible Endoskopie durchgeführt.
Erst Wochen später wurde eine junge Ärztin in der HNO-Chirurgie Karlsruhe aktiv und führte eine einfache flexible Endoskopie durch die Nase durch. In Vorbereitung einer UPPP. Fast erschrocken zog sie den Oberarzt hinzu. OT des Oberarztes „ein so enges Velopharynx hat er bisher noch nicht gesehen.“ Die für den nächsten Tag geplante OSA-Operation vom Typ UPPP der Karlsruher HNO-Chirurgie wurde daraufhin verworfen, weil diese Methode der Uvulopalatopharyngoplastik (UPPP) nicht geeignet erschien, meine Atemwegsverengung dauerhaft zu beseitigen. Im Arztbrief wurde auf die Möglichkeiten der Kiefer-Chirurgie (OSA-Dysgnathie-OP) verwiesen. – Danke –
-
Endoskopie der Atemwege
Endoskopie der Atemwege
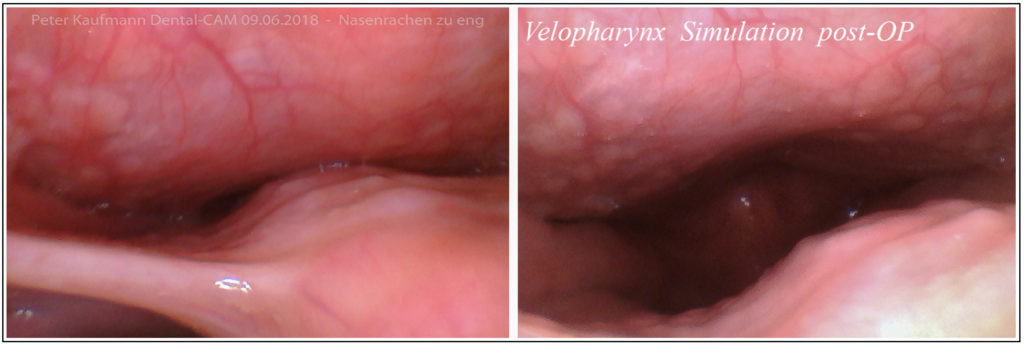
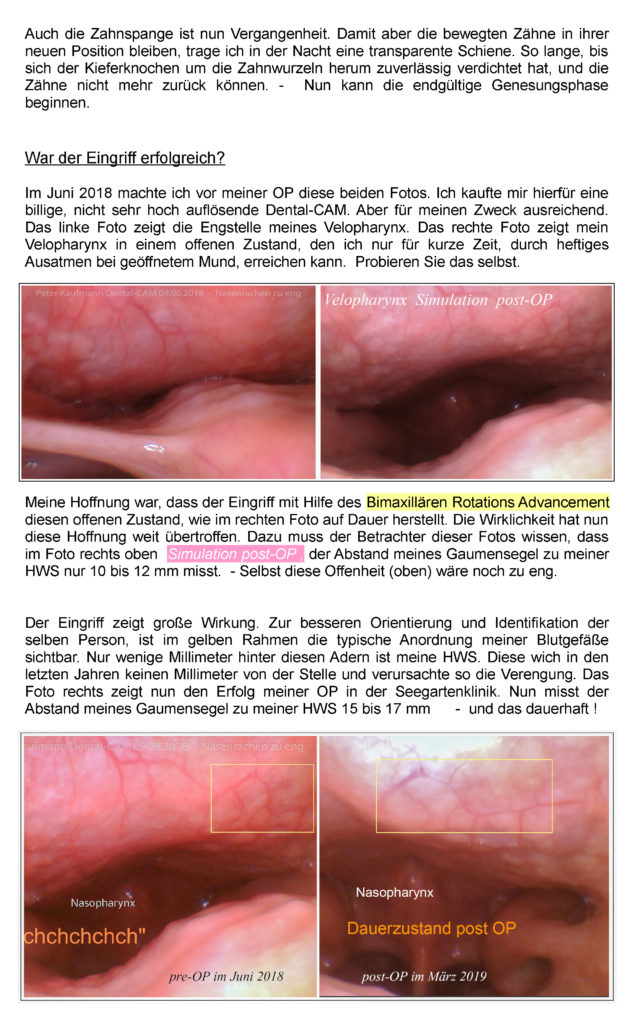
Beide Fotos zeigen mein Velopharynx. Die Mini-Kamera blickt von der Zunge nach oben in den Nasenrachenraum (Nasopharynx). Im linken Foto ist der enge Dauerzustand bei entspanntem Gaumensegel zu sehen. Das Foto rechts zeigt eine provozierte Offenheit meines Velopharynx. Diesen Zustand kann ich nicht dauerhaft halten. Dieser offene Zustand kann nur bei starker und schneller Ausatmung bei geöffnetem Mund provoziert werden.
So wie im rechten Foto zu sehen, wird es hoffentlich nach der Vorverlagerung incl. einer Rotation meines Oberkiefers (Bimaxilläres Rotation Advancement) aussehen. Daher die Kennzeichnung mit Simulation post-OP. Eine einfache Vorverlagerung um nur wenige mm ohne Rotation wird nicht ausreichen mein Velopharynx zu vergrößern. Das hat seinen Grund in der Trägheit, mit der die Weichteile einer Vorverlagerung des Ober- und Unterkiefers folgen können.
Beide Fotos wurden im Sitzen gemacht. In der Nacht in Rückenlage verschließt sich die Engstelle (linkes Bild) wie ein Rückschlagventil, und eine Ausatmung ist nicht möglich. Die bereits im Januar 2018 verordnete CPAP-Therapie konnte die Apnoen, Hypopnoen und Flusslimitierungen nicht zufriedenstellend verhindern. Stundenweise nahmen diese sogar zu. Zeitweise hatte ich unter CPAP-Therapie über die Dauer von 45 Minuten einen Apnoe-Index von 30. Mit den Hypopnoen ein AHI von 45. In absoluten Zahlen ausgedrückt verbrachte ich 8 Minuten in Apnoe während 45 Minuten CPAP-Therapie. Die längste Apnoe 38 Sekunden.
Statistik ist wunderbar, aber relativ. Das CPAP dokumentierte am Morgen einen AHI von 12. Nach dem Aufstehen fühlte ich mich kaputt, müde und antriebslos. Trotz CPAPTherapie. Die Auswertung der CPAP-Daten zeigte aber auch, dass Flusslimitierungen und Hypopnoen, die einzeln unter 10 Sekunden andauern, sich zusammen aber über Stunden erstrecken, oder Apnoen vorausgehen, im AH-Index nicht erfasst werden. Ein Schlafmediziner aber, der CPAP liebt, schaut sich meine Daten im einzelnen nicht an! Er vertraut seiner Statistik. – Statistisch habe ich mit CPAP relativ gut geschlafen, – tatsächlich aber eher schlecht. -
Empfehlung des Klinischen Schlaflabors Karlsruhe
Empfehlung des Klinischen Schlaflabors Karlsruhe
Nach der HNO-Chirurgie Karlsruhe schrieb nun auch der Oberarzt des Klinischen Schlaflabors Karlsruhe in seinem Arztbrief zur CPAP-Therapie und deren Versagen eine Empfehlung für eine Kieferchirurgische Dysgnathie-OP.
„Schlaf gestört bei erhöhtem Arousal-Index v. 35 pro Std. Eine CPAP- Steigerung wegen relevanter Flusslimitierung und obstruktiver Hypopnoen brachte keinen Erfolg. Eine geplante HNO-Chirurgische OP in Karlsruhe wurde wieder verworfen. Im Rahmen einer Kieferchirurgischen Untersuchung zeigte sich in der Bildgebung (Digitale-Volumen-Tomographie) eine Einengung des retropalatinalen Raumes. Möglicherweise kann ein kieferchirurgischer Eingriff die nächtliche Atemsituation bessern. Mit freundlichenGrüßen“ / gez. Oberarzt (Juni 2018).
-
Bimaxilläres Rotation Advancement
Bimaxilläres Rotation Advancement
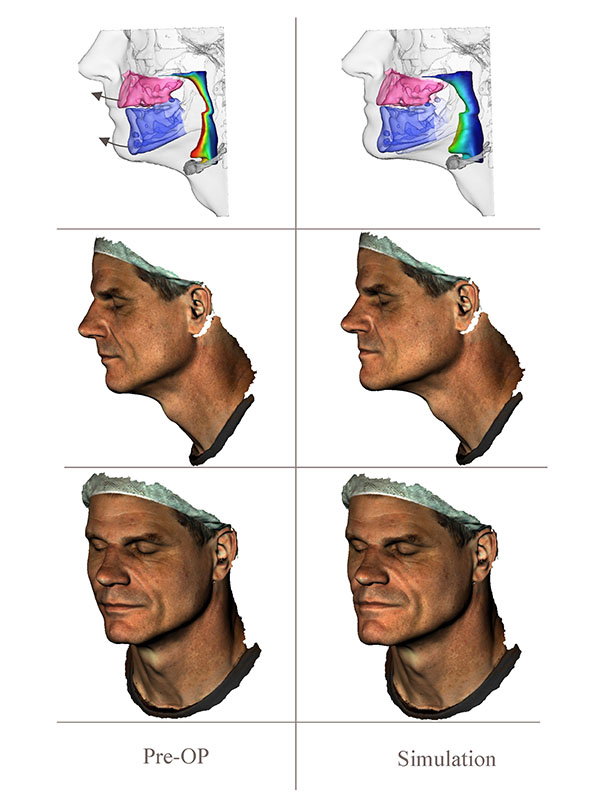
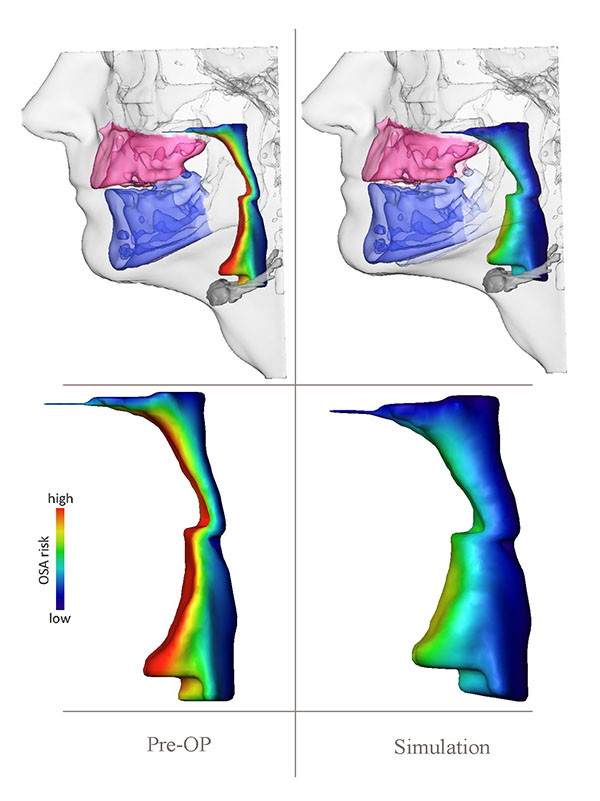
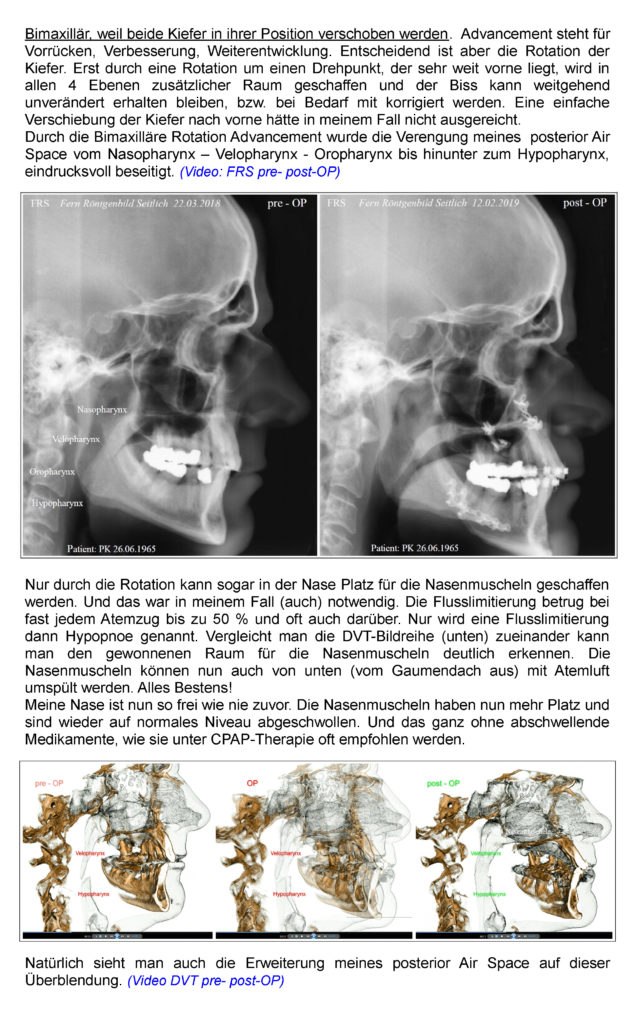
Zuvor hatten wir über die Möglichkeiten einer Bimaximillären-Rotation-Advancement Operation in der Seegartenklinik Heidelberg gesprochen. Bimaxillär, weil beide Kiefer in ihrer Position verschoben werden. Advancement steht für Vorrücken, Verbesserung, Weiterentwicklung. Entscheidend ist aber die Rotation der Kiefer. Erst durch eine Rotation um einen Drehpunkt, der sehr weit vorne liegt, wird in allen 4 Ebenen zusätzlicher Raum geschaffen und der Biss kann weitgehend unverändert erhalten bleiben, bzw. bei Bedarf mit korrigiert werden. Eine einfache Verschiebung der Kiefer nach vorne hätte in meinem Fall nicht ausgereicht. Durch die Bimaxilläre Rotation Advancement wurde die Verengung meines posterior Air Space vom Nasopharynx – Velopharynx – Oropharynx bis hinunter zum Hypopharynx, eindrucksvoll beseitigt.



3D Planung